
Photo by Age Cymru on Unsplash
End of life care in long term care settings begins before death occurs. As a resident declines, caregivers may notice physical, mental, behavioral, and emotional changes that signal the final stage of life is approaching.
Recognizing these changes matters for three reasons. It helps caregivers respond appropriately, keeps the resident as comfortable as possible, and prepares loved ones for what is happening.
This guide explains common end of life signs, what comfort-focused care looks like, how hospice fits in, and how to support families during and after a death.
What end of life care means in long term care
End of life care is care focused on comfort, dignity, and peace when a person is nearing death. In long term care, this often includes close observation, updating the care plan as needs change, honoring the resident’s wishes, and helping loved ones understand what to expect.
Each person’s dying process is different. Not every resident will show the same signs, and the timing can vary. Still, a growing number of clinical signs often indicates the person is nearing the end of life.
Why early recognition is important
When decline is recognized early, caregivers and the care team can:
Adjust the resident’s assessment and care plan
Discuss and document final wishes when requested
Increase comfort measures
Educate loved ones about expected changes
Coordinate with hospice or the resident’s clinician
Early recognition also helps avoid misunderstandings. Changes such as reduced eating, sleeping more, confusion, or altered breathing can be distressing to families if they are not explained clearly and calmly.
How functional decline may be assessed
Some clinicians use the Palliative Performance Scale to measure functional decline and help predict survival in people with serious illness. This tool looks at five areas:
Ambulation
Activity level and evidence of disease
Self care
Oral intake
Level of consciousness
It may also help clinicians make informed decisions about hospice eligibility.
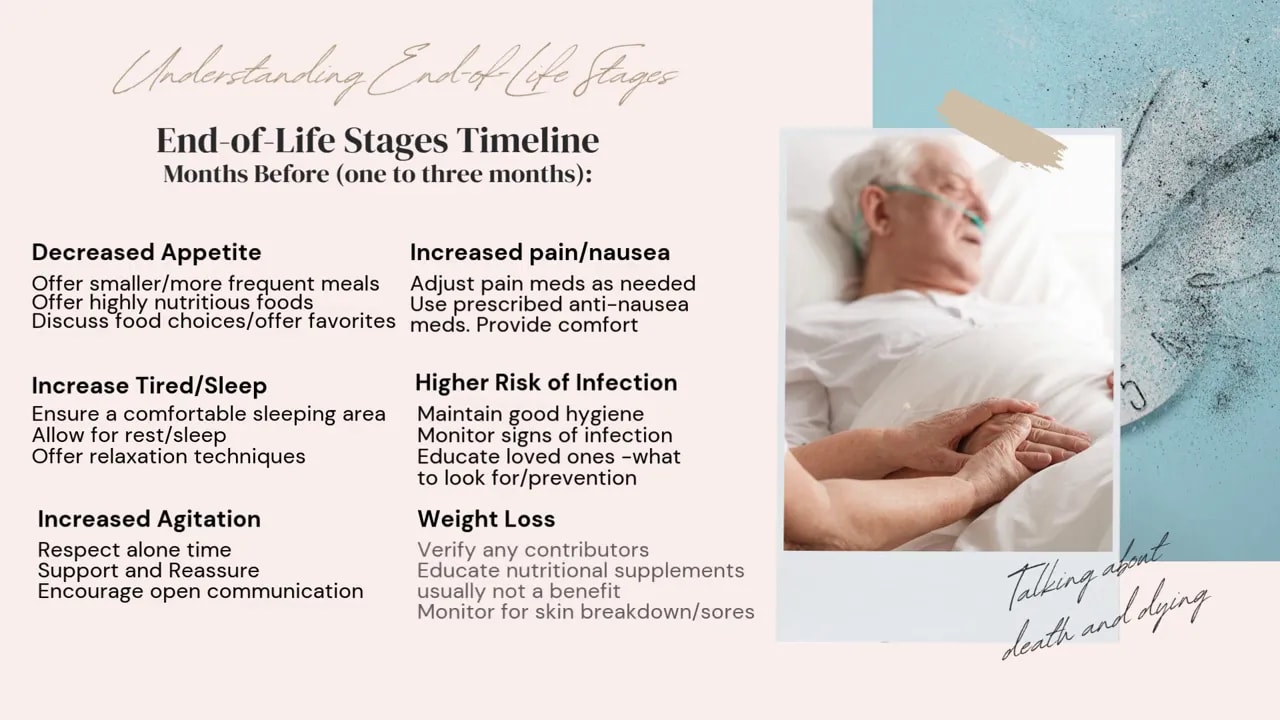
Common end of life signs months before death
In the final one to three months, residents may begin showing broad signs of decline. These can include:
Decreased appetite
Increased pain or nausea
More tiredness and sleeping
Higher risk of infection
Increased agitation
Weight loss
Comfort measures during this stage
Offer smaller, more frequent meals
Provide nutritious foods and favorite foods when desired
Follow medical orders for pain and nausea treatment
Create a comfortable space for rest and sleep
Maintain good hygiene and watch for infection
Respect requests for time alone
Monitor for skin breakdown and sores, especially with weight loss
Common end of life signs in the final weeks
In the weeks leading up to death, changes usually become more noticeable. Common signs include:
Increased need to sleep
Little or no interest in eating
Agitation
Restlessness
Congestion
Confusion
Hallucinations or visions
Vital sign changes
How to care for a resident in the final weeks
If the resident is sleeping more:
Allow rest
Keep the sleeping area comfortable
Explain the sleep changes to loved ones
If the resident no longer wants food:
Respect the choice to eat or not eat
Offer sips of fluid if appropriate
Provide mouth care to prevent dryness
Report refusal to eat to the resident’s clinician
If the resident is restless:
Check for possible causes
Reposition for comfort
Use calming or relaxation techniques
If congestion increases:
Elevate the head for easier breathing
Use a humidifier if appropriate
If confusion increases:
Use clear, simple explanations
Use visual cues if needed
Keep the environment calm and quiet
If hallucinations or visions occur:
Reassure the resident
Offer support
Acknowledge the experience without arguing
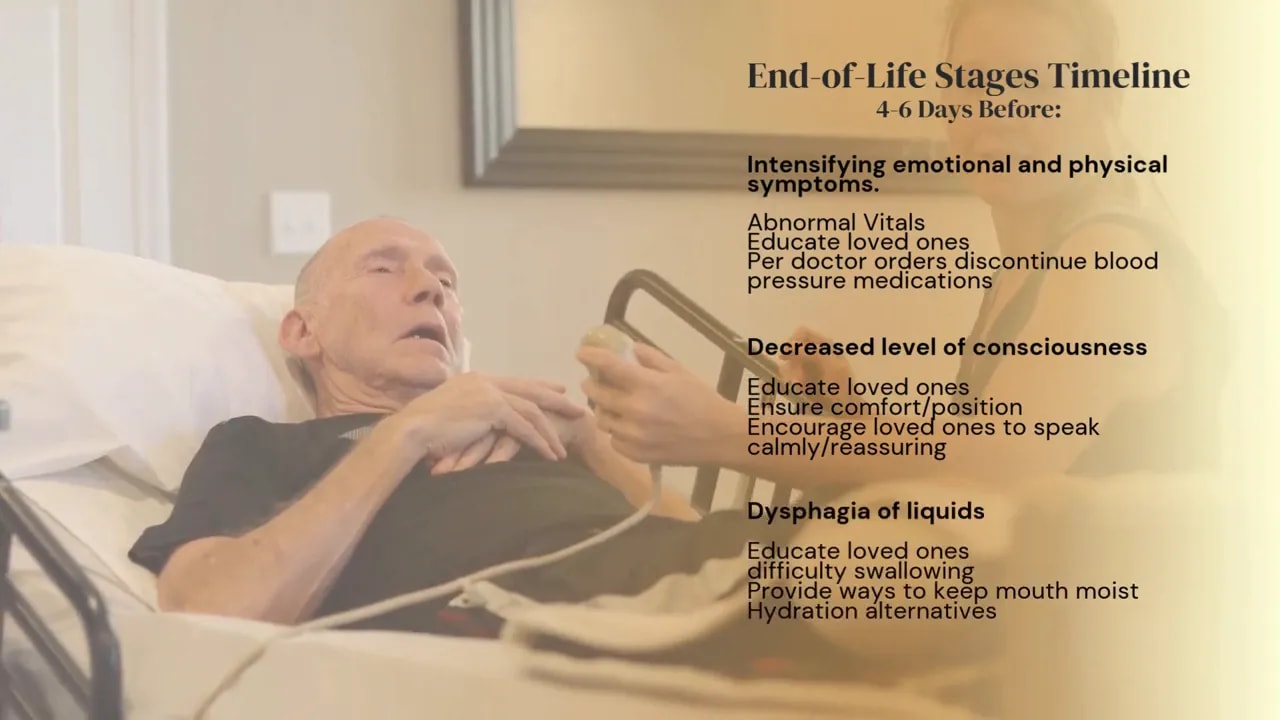
Signs that death may be a few days away
About four to six days before death, symptoms may intensify. Residents may show:
Abnormal vital signs
Decreased level of consciousness
Difficulty swallowing liquids
At this stage, caregivers should focus on comfort and education. Mouth moisture becomes especially important when swallowing is difficult. Loved ones often need reassurance that these changes can be part of the normal dying process.
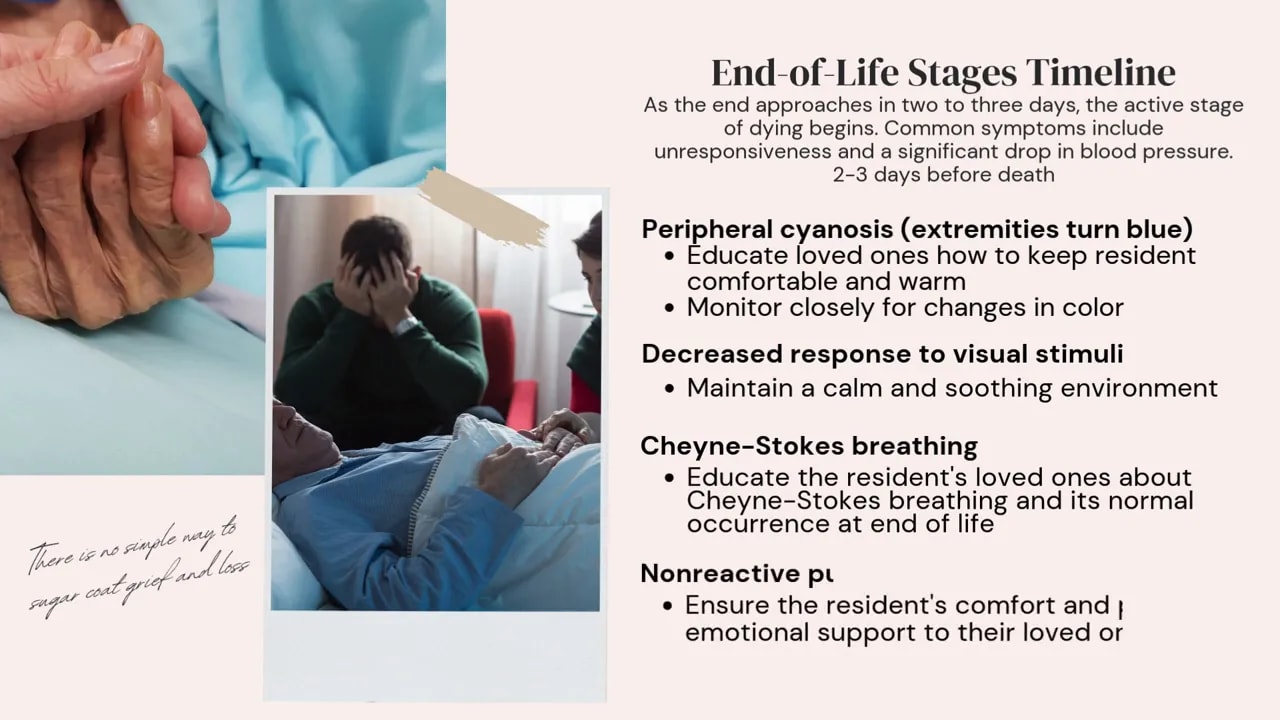
Active dying: signs in the last two to three days
The active stage of dying often begins about two to three days before death. Common signs can include:
Unresponsiveness
A significant drop in blood pressure
Peripheral cyanosis, where the hands, fingers, toes, or nose may look bluish or dusky
Less response to visual stimuli
Cheyne-Stokes breathing, with alternating deep breathing, shallow breathing, and pauses with no breathing
Fixed or dilated pupils
How to respond during active dying
Keep the resident warm and comfortable
Maintain a calm, soothing environment
Educate loved ones about color changes and breathing changes
Provide emotional support
Coordinate with hospice or the clinician regarding symptom relief
Cheyne-Stokes breathing can be alarming to families. It is important to explain that this breathing pattern is a normal occurrence at the end of life.
Final hours: what caregivers may notice
In the final hours, several specific signs may appear:
Death rattle, a wet or gurgling sound caused by secretions in the upper airway
Decreased urine output
Pulselessness of the radial artery
Eyes that do not fully close
Grunting from vocal cord tension
Fever
Comfort measures in the final hours
Reposition the resident to help drainage if secretions are present
Use a wet washcloth if the eyes are dry or irritated
Give prescribed medication if pain is present
Use a cool washcloth on the forehead for fever
Remove excess blankets and use a fan if appropriate
Administer acetaminophen only if needed and prescribed
The death rattle often worries loved ones, but it usually does not mean the resident is in pain or discomfort. Clear explanation can reduce fear in the room.
Mental, emotional, and behavioral changes near death
Clinical signs are only part of the picture. Mental and emotional changes can also signal that a resident is approaching death.
Common changes may include:
Excessive fatigue
Long periods of sleep
Confusion or disorientation
Hearing or seeing people or events that others do not perceive
Social withdrawal and detachment
Life review, reflecting on the past
A desire to settle unresolved matters
Interest in funeral planning
Withdrawal is common. A resident may decline visits from friends, neighbors, or even family members. When visits do occur, interaction may be limited. This can feel personal to loved ones, but it is often part of the natural process of separating from the world around them.
How culture and gender may affect end of life conversations
Social, cultural, and religious factors shape how people experience dying. Some individuals want practical facts and direct discussion. Others may avoid the topic or prefer a more gentle approach. Religious and cultural beliefs may strongly influence decisions, rituals, and how openly death is discussed.
Caregivers should avoid assumptions. Instead:
Ask respectful questions
Honor stated preferences
Support meaningful rituals when possible
Communicate with empathy and clarity
What hospice is and when it may begin
Hospice supports people near the end of life. It may be provided in a private home, adult foster care facility, home for the aged, nursing home, rehabilitation facility, hospital, or hospice center.
The goal of hospice is to improve quality of life by focusing on comfort and peace rather than curing the serious illness.
Hospice care is typically available to residents with a life expectancy of six months or less.
What changes when hospice starts
When hospice begins, treatments meant to cure or control the serious illness stop. For example, chemotherapy would end before entry into hospice. However, the resident may still receive medications for other conditions or symptoms, such as blood pressure treatment or symptom relief medications.
What hospice does not always mean
Hospice does not usually mean a staff member is physically present 24 hours a day, 7 days a week. In many settings, the long term care team still provides much of the hands-on day-to-day care. A hospice team member should still be reachable by phone at all times.
Key caregiver responsibilities when a resident is on hospice
If a resident in long term care is receiving hospice services, caregivers should be prepared to provide proper end of life care between hospice contacts. That includes:
Monitoring changes closely
Keeping the resident comfortable
Administering prescribed medications as ordered
Communicating changes promptly
Educating loved ones about what is normal at end of life
Important DNR and emergency response considerations
Do not resuscitate rules can be complex in long term care settings. Caregivers must know and follow the administrative and licensing rules that apply in their setting.
One key point from the source material is this: in an adult foster care setting, a licensee cannot independently honor a do not resuscitate or no-code request outside the specific framework described in licensing rules and the hospice service plan.
For a resident enrolled in a licensed hospice program with a do not resuscitate order in the hospice service plan:
If the resident has a serious adverse medical change, the facility should contact the licensed hospice provider immediately instead of emergency medical services.
If the resident is involved in an accident and needs emergency medical care, staff should contact emergency medical services immediately and then notify the hospice program.
Because these rules are highly specific, caregivers should never rely on assumptions. Follow the resident’s plan, facility policy, and applicable state requirements.
How to support loved ones before and after death
Support for loved ones is an essential part of end of life care. The circumstances surrounding a death often become lasting memories, so the environment and communication matter.
What helps families most
Give private time to say goodbye and share memories
Answer questions factually and calmly
Explain what will happen next in the coming hours or days
Honor rituals such as prayers, bathing the body, or special clothing when appropriate
Keep the space clean, orderly, and free of offensive odors
Families should not be subjected to avoidable stress during this time. Small details such as privacy, cleanliness, and clear communication can make a major difference.
Supporting the grieving process
Grief is individual. It does not follow a simple schedule, and it can rise and fall over days, weeks, months, and years.
Caregivers can support healthy grieving by:
Being empathetic
Avoiding judgment about how someone is grieving
Respecting cultural and religious practices
Using calm, compassionate language
If the resident was receiving hospice care, Medicare-certified hospices may provide up to one year of grief and loss counseling for loved ones after the resident’s death.
Common mistakes to avoid in end of life care
Forcing food or fluids when the resident no longer wants them
Arguing about hallucinations or visions instead of offering reassurance
Treating normal end of life breathing changes as automatically painful without assessing the whole situation
Failing to report important changes to the nurse, clinician, or hospice team
Ignoring requests for privacy, rituals, or final wishes
Assuming hospice staff are always physically present
Making assumptions about DNR procedures instead of following policy and applicable rules
Quick end of life caregiver checklist
Watch for changes in appetite, sleep, breathing, alertness, and comfort
Update the care plan as needs change
Keep the resident clean, warm, calm, and positioned comfortably
Provide mouth care regularly
Administer only prescribed medications as ordered
Explain expected changes to loved ones in simple language
Honor final wishes and meaningful rituals when possible
Contact hospice or the clinician promptly when changes occur
Know facility rules for emergencies and do not resuscitate orders
Allow private time and support grieving after death
Takeaway
Good end of life care in long term care is not only about recognizing the final physical signs of dying. It is also about preserving dignity, reducing distress, respecting wishes, and helping loved ones move through a difficult experience with clarity and support.
The most important caregiver skills at the end of life are close observation, comfort-focused care, calm communication, and compassion.